Achieving BP Indicators
Introduction
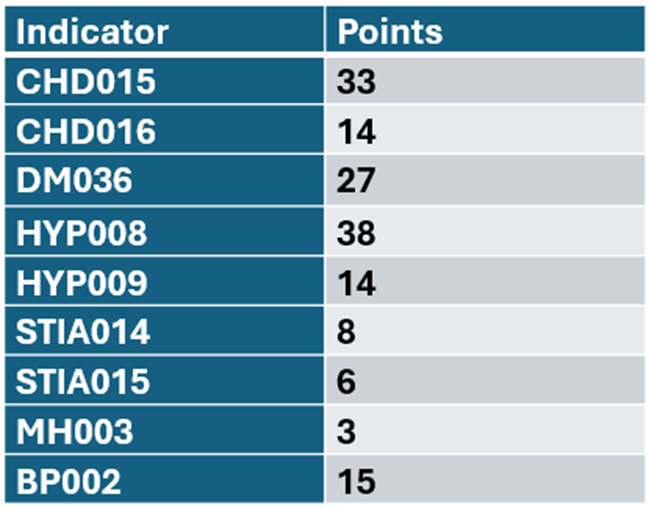
A number of QOF indicators require a patient to achieve a blood pressure target and for 2025/26 these indicators have been particularly important for income as they are worth a total of 140 points. There are also two indicators requiring a BP but with no target for the results – MH003 which requires an annual BP (worth 3 points) and BP002 which requires a BP reading every 5 years (worth 15 points). For a practice with an average list size and prevalence this means that BP indicators overall are worth approximately £35k.
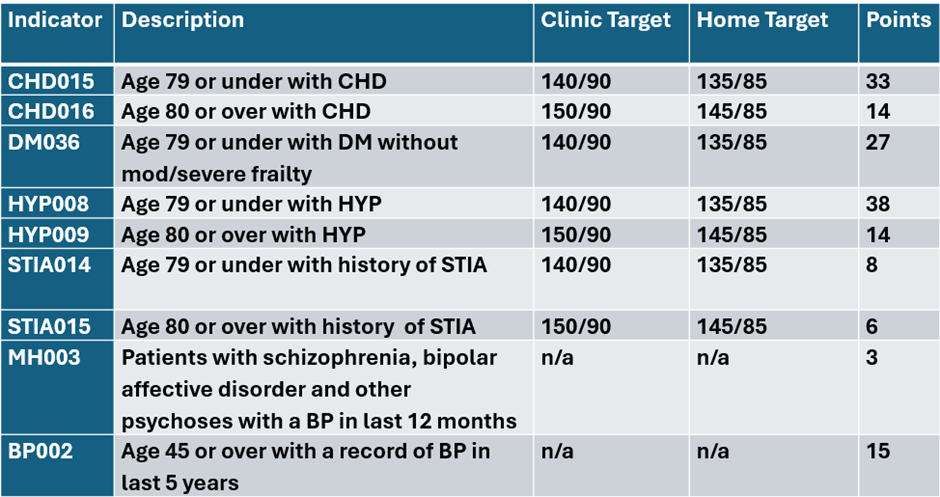
The BP Indicators:
Achieving maximum points for these indicators can be difficult due to the way targets are measured for the achievement. There are lower targets for readings taken at home by the patient and those taken in a clinical setting or by a clinician, there are also rules around invitations and PCAs that can make a significant difference to end of year results.
The redistribution of QOF points for 2025/26 and increased focus on CV prevention means that these indicators have a much more significant impact on QOF income.
Key areas to consider:
– Use all available resource
– Ensure the whole team knows the targets
– Identify outstanding patients on multiple registers
– Identify borderline patients
– Consider Quick Wins
– Consider PCAs
Know The BP Targets
A practice’s blood pressure protocol will often involve the whole practice team. Clinicians need to be aware of targets so that they can record clinical interventions and personalised care adjustments to reflect a patient’s management plan, non-clinical staff are often involved with recording blood pressure readings taken at home or coming from 3rd party providers such as pharmacies and encouraging and supporting patients to use BP machines or pods in reception areas.
Patients will often have multiple BP readings throughout the year and results may fluctuate. This means that a patient who has met the target early in the year may then have another reading later in the year that fails the target and moves them back to the excluded list.
The only exceptions to this are MH003 which just requires an annual BP and BP002 which is a public health indicator and only requires the patient has a BP recorded at least every 5 years.
Targets
Make sure the team is aware that:
– Targets are 5mmHg lower for BPs recorded at home
– The latest BP reading is the one that will count at the end of the year
– If recording a BP above target consider – is there a plan to bring this down OR is there a reason not to try and bring it down
– Patients can be on multiple registers
– The pink box will make it clear when a patient is not meeting a QOF BP target
It is essential to have a clear BP protocol for the practice which is followed by the whole team. Especially important for non-clinical staff recording BPs to ensure they are escalating results as per a written protocol rather than making a decision without appropriate training. This is not just important for QOF but something that CQC may wish to review especially with the current focus on CV prevention.
Identify outstanding patients who affect multiple indicators
Patients often fall into more than one cohort for BP indicators. A patient with diabetes may also have hypertension. A patient may have coronary heart disease and also have a history of a stroke or TIA. Practices will usually even have some patients who have hypertension, diabetes, coronary heart disease and a history of stroke or TIA.
Consider targeting patients who are currently outstanding and who affect 3 or 4 indicators especially if the practice has not yet hit targets in more than one indicator.
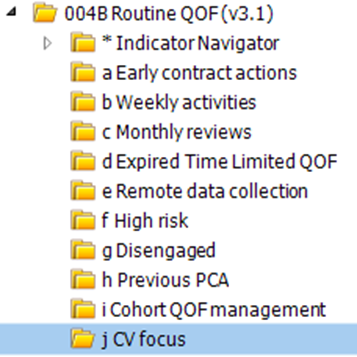
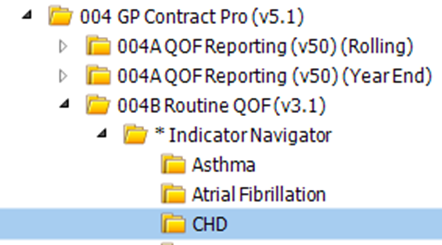
PCIT offers searches to support the practice with identifying these patients in the CV focus folder which can be found on 004B Routine QOF – j.CV focus
In this folder, the patients with outstanding BPs have been broken down into 4 groups:
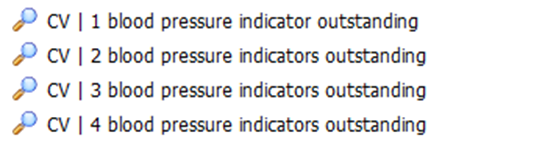
The practice can then choose to start with those who have 4 indicators outstanding, recording a new BP for these patients which meets the target or recording a PCA for these patients will then impact the results of all 4 indicators.
If reviewing patients on multiple indicators remember some PCAs are applicable across the indicators and other PCAs are indicator specific. See the section below for more information on PCAs and BPs.
Identify Borderline Patients
Patients with borderline BP results often move between the ‘included’ and ‘excluded’ results throughout the year. They may also have been assessed by a clinician as having a satisfactory BP from a clinical standpoint or have reasons why a targeted approach to reducing their BP may not be appropriate.
The CV Focus folder has 2 reports which combine all the BP indicators to produce a list of patients who have had a BP recorded this year but are not to target. Note that these reports exclude patients with a history of PCAs in previous years such as maximum tolerated antihypertensives, informed dissent or clinically unsuitable as there are separate searches to review those patients.
The CHECK BORDERLINE searches in CV Focus will show all patients but the report is designed to be exported into Excel and sorted or filtered. This allows practices to decide what they consider to be borderline and which patients should be prioritised for review.
The Indicator Navigator searches in 004B also include BORDERLINE searches that are aimed at patients who have had a home BP recorded that did not meet the home BP target but that would have met the clinical BP target. Practices may wish to review these patients to consider whether to offer appointments for a follow-up clinical BP or encourage them to use in-house BP machines or pods.
For example these searches in the Hypertension folder:

The searches that look for a BP this year that is not to target with no previous PCA are also replicated in the individual disease register folders under Indicator Navigator. If a practice only needs to work on achieving a particular BP indicator in Q4 they may wish to use the indicator specific versions to target a smaller cohort of patients.
Consider Quick Wins
The Indicator Navigator folders for individual disease registers include Quick Win searches for BP indicators.
These will provide a list of outstanding patients who have not had a BP recorded yet this year but whose latest BP on record was within the target range.

As with all reports, this has been designed to present the information at a glance so that it can be opened in Excel and ordered to suit the practice. Some practices may wish to target patients with the most recent BP or others may wish to start with those whose last BP was particularly good.
If choosing to send additional invites to these patients it is important to consider the impact if they respond and have a BP reading done that is not within target. If they have already had 2 invites they will not currently be included in the denominator which means they are not adversely affecting the practice’s achievement. If they then attend and have a BP that is above the target they will move to the ‘excluded’ list and will then adversely affect the achievement unless another PCA is applied or a further 2 invites are sent before the end of the QOF year.

Consider PCAs
PCAs (Personalised Care Adjustments) are rules that remove patients from the denominator for a particular indicator. The denominator is the parent population for that indicator so applying an appropriate PCA means that patient will not count against the achievement at the end of the year.
The majority of clinical indicators in QOF have ‘area of care’ PCAs which affect all indicators in that disease area:
Informed dissent – patient has declined to be reviewed or have the relevant monitoring
Patient unsuitable – patient is clinically unsuitable
There is also an automatic PCA applied when a patient has had 2 invitations sent at least 7 days apart. Invitation codes can be specp6ific to the disease area or there are also generic invitation codes for practices who invite people for holistic reviews looking at all QOF areas. The generic invite codes can also be useful if sending a BP invite to patients on multiple registers. Just be aware that invite codes apply to the whole disease area, not just the BP indicators.
Each QOF indicator may then have additional PCAs. All PCAs are listed in PCIT’s QOF Indicator Support articles which can be accessed here Contractual Support | QOF Indicator Support Knowledge base
For BP indicators, key PCAs are:
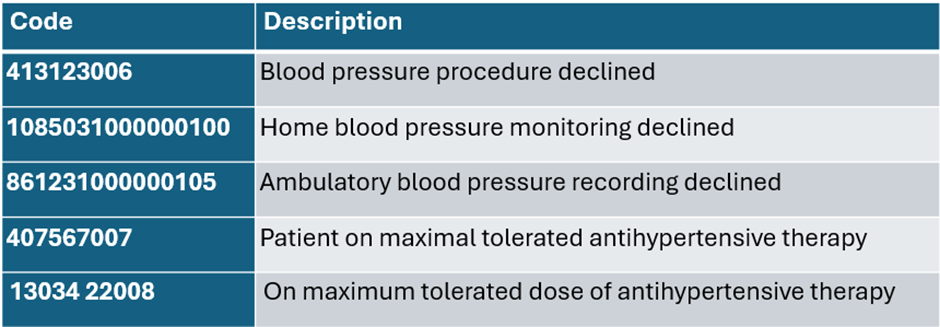
Note: a change to the SNOMED coding for maximum tolerated therapy means that there are currently two potential codes for this. Only one code can be selected in the code browser but the older “maximal” code is still available in templates.
Both codes are included in the QOF business rules for 2025/26.
Cardiovascular disease prevention is a priority area for many reasons. Don’t just think about achieving these indicators for Q4 but make sure to include all of these areas in the practice plan for 2026/27.
📹 Thank you to everyone who joined us for our “Wondering about QOF at this time of year?” webinar yesterday. For customers, this was a refresh of our GP Contract Pro tools, particularly focusing on actions to tidy up QOF at this time of the year.
This webinar showed PCIT resources but is suitable for both customers & non-customers utilising either EMIS Web or TPP SystmOne.
🌐 Watch here: Wondering about QOF at this time of year? on Vimeo