QOF Indicators Requiring Reviews
Introduction
Annual reviews are a core part of QOF and often have the biggest impact on staff workload and clinic capacity. Having a clear practice protocol for recalls, a team approach and ensuring accurate coding throughout can make a big difference to achievement at the end of the year.
In Q4 it is important to ensure that all completed work is contributing to the indicator achievement and that the practice has a clear priority list and plan for mopping up any remaining points. A practice wide plan is key for review indicators to ensure everyone is working towards a common goal and that remaining appointment capacity is used as efficiently as possible to maximise QOF income.
Indicators:
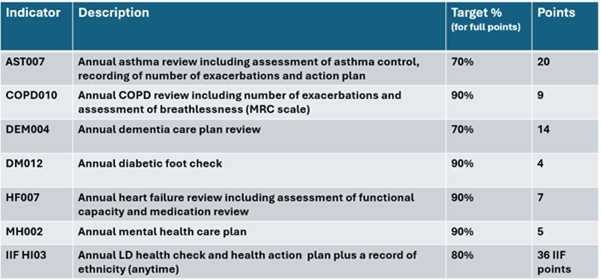
AST007 – Annual asthma review including assessment of asthma control, record of exacerbations and written action plan.
More details – AST007 – Asthma annual review
COPD010 – Annual COPD review including number of exacerbations and assessment of breathlessness (MRC)
More details – COPD010 – COPD review
DEM004 – Annual dementia care plan review
More details – DEM004 – Dementia care plan review
DM012 – Annual diabetic foot check
More details – DM012 – Diabetic foot risk classification
HF007 – Annual heart failure review including assessment of functional capacity and medication review.
More details – HF007 – Heart Failure review
MH002 – Annual mental health care plan
More details – MH002 – SMI care plan
HI03 (IIF) – Annual Learning Disability health check and health action plan plus record of ethnicity
More details – HI03 – % of patients with LD with health check with health action plan and recording of ethnicity
Key areas to consider:
· Coordinate the team
· Combine reviews
· Consider accessibility
· Ensure appropriate staff know the QOF requirements
· Ensure all staff are aware of importance of booking before 31st March
Coordinate the team
Annual reviews can often end up being left to specific members of the team to manage, such as a nurse specialising in diabetes doing all the foot checks as part of an annual review. However, this can mean patients who are eligible for multiple indicators end up attending for multiple separate appointments which increases pressures on staffing capacity.
Many practices have moved to a holistic, combined annual review system covering multiple QOF areas in one appointment (depending on the patient). Planning to move to a combined annual review approach will depend on staff being trained in multiple specialist areas, so this may be considered as part of a strategic long-term practice plan. For practices who use a birthday month system it is important to ensure that patients whose birthday falls in Q4 (January-March) are invited in time to allow for booking and attending a review before 31st March, and that the recall plan includes sending 2 invites in the first part of Q4 so that outstanding work is clear.
Separate annual reviews can still include elements that contribute to other disease areas so it is important that staff doing those reviews are aware of the requirements that may overlap. For example, a heart failure review does not specifically require a blood pressure check but including a BP check in the appointment may tick the box for other indicators.
This is especially important to consider in Q4 when there is limited time and appointment availability before 31st March. So a team approach is essential to achieving those last few points.
Practices should also ensure that staff responsible for booking appointments are aware of the 31st of March deadline and practice priorities for review appointments. If the practice has not yet achieved full points for DM012 then staff may need to highlight if they are struggling to fit in any more diabetic foot checks with the appropriate member of the team. The practice can then consider if any adjustments need to be made to clinics to accommodate fitting in foot checks.
Know The Requirements
QOF review indicators have two types of ‘requirements’ that should be considered.
First there are the essential required elements where a code is required for the review to count towards the QOF achievement. Failing to code an essential element is a common problem that may lead to patients receiving multiple invites despite having already attended for their review earlier in the year or even being booked in for more than one annual review.
Secondly there are the clinical recommendations listed within the QOF guidance and linking back to NICE guidance. It is important to look at these as coding that a review has happened where the review does not meet these recommendations may be questioned if audited.
To identify patients who may have attended for review, but who are not currently contributing to the achievement due to missing codes the PCIT 004 GP Contract Pro/ 004B Routine QOF work | Indicator Navigator folder includes a number of DQ or ‘data quality’ searches for each disease.
AST007 Asthma Review –This indicator includes essential elements that also need to be coded within a specific time frame relative to the review.
It is essential to code:
o Asthma review
o Written asthma care plan coded on the same day as the review
o Number of exacerbations coded up to 1 month before or on the same day as the review
The written asthma care plan must be coded on the same day as the review. The recording of the number of exacerbations must be coded up to 1 month before or on the same day as the review. In 004 GP Contract Pro / 004B Routine QOF work | Indicator Navigator – AST | DQ | Asthma with incomplete review will show these outstanding elements.
COPD010 COPD Review – This also needs a record of the number of exacerbations and assessment of breathlessness using the MRC scale. Unlike asthma, these elements do not need to be within a certain timeframe around the review and just have to be coded at any point in the QOF year.
Essential to code:
o COPD review
o Number of exacerbations
o Assessment of breathlessness (MRC scale)
Again, the 004B Routine QOF work | Indicator Navigator folder for COPD offers a report to help quickly identify missing elements so they can be actioned before 31st March.
DEM004 Dementia Care Plan –The essential element for this indicator is a code showing a dementia care plan has been agreed or reviewed. There is not a requirement to code a dementia review alongside this.
However, the QOF guidance indicates that this care plan is expected to be part of a formal review which should include a number of other elements including:
· Physical, mental health and social assessments
· Medication review
· Record of patient’s named coordinator or key worker and contact info
· Record of any legal power of attorney in place
· End of life preferences with consideration to whether patient should be on the palliative register
· Review of NICE recommended interventions
· Identification of patient’s carer and offer of a carer health check if appropriate
The codes for these elements are not explicitly required for the patient to be included in the QOF indicator achievement and would depend on the needs of the patient. The dementia page of the QOF template offers coding options for all of the above elements. The clinician performing the review should be aware of the QOF and NICE guidance to ensure the review and associated care plan covers all appropriate elements.
DM012 Diabetic Foot Check –This indicator has a single essential element which is the diabetic foot check. There is no requirement for an annual review alongside this. Be aware that this indicator is due to change in 2026/27 so look out for information on this with the 2026/27 QOF Update.
HF007 Heart Failure Review – This indicator requires a heart failure review and a medication review both within the QOF year. There is no requirement for the medication review to be on the same date or close to the review.
It is essential to code
o Heart failure review
o Medication review
The Indicator Navigator HF searches identify patient who have had one of the essential elements coded but are missing the other code.
Much like DEM004 there is an expectation that the heart failure review is conducted in line with NICE recommendations. The QOF guidance specifically recommends evidence of an assessment of functional capacity. The Heart Failure page of our QOF template provides the appropriate New York Heart Association Classification codes to support this, but these are not essential codes for achievement of the indicator.
MH002 Mental Health Care Plan – This indicator requires a single code indicating that a care plan has been agreed or reviewed within the QOF year.
For patients on this register the care plan is often part of wider multidisciplinary support, and the QOF guidance does allow for documenting of a care plan that has been reviewed by community health services if the patient is under their care. If the patient is not under the care of community health services, then the guidance advises that the care plan should be part of a primary care consultation.
TOP TIP – Make sure that coders are aware of the need to code care plans agreed or reviewed by the community mental health team to avoid duplication of work.
Although the care plan may be agreed or reviewed outside of an annual health check it is often useful to consider the combined mental health indicators as an annual review for the purposes of planning.
HI03 (IIF) Learning Disability Health Check – This is an IIF indicator rather than a QOF indicator, but it is important to include it when planning annual reviews.
This indicator has 3 essential elements:
· A learning disabilities health assessment in the QOF year
· A review or completion of a LD health action plan in the QOF year (must be done on the same date or after the health assessment, not before)
· A record of ethnicity (does not need to be repeated each year)
IIF searches are in folder 025 PCN Contracts with IIF Reporting searches showing achievement and IIF Data Quality has searches identifying patients who have had the assessment or action plan coded but have not had all 3 essential elements recorded.
PCIT QOF template
PCIT offers a dedicated QOF template designed to streamline your workflow and support accurate achievement across each disease area. This template includes only the essential clinical codes required to meet QOF indicators, helping to keep consultations focused, efficient, and compliant. Each disease area has been separated into its own dedicated page, and the template intelligently displays only the conditions relevant to the patient record retrieved. By removing unnecessary fields and codes, this approach helps reduce errors, minimise incorrect coding, and create a clearer, more user-friendly experience.
To further support clinical decision-making, each disease area includes a dedicated view displaying key patient information relevant to that specific indicator. PCIT has also included quick links to a detailed exception reporting template, containing all appropriate exception codes alongside a tailored view to support safe and informed exception reporting. In addition, users can access a more comprehensive condition-specific template directly from each disease page, making it easy to move from focused QOF coding to a full, in-depth review whenever required.
Identify outstanding patients
In Q4 it is important to have a targeted approach to identify patients who are outstanding and currently affecting the practice’s potential achievement.
The first step is to make sure that any Data Quality reports have been reviewed and actioned to check that patients have not already attended for a review. This helps to avoid sending recalls when the work has already been done.
Once the Data Quality report has been reviewed and actioned, the next step is to ensure that all remaining patients have had 2 invitations. This will mean that any patients who do not attend for a review by 31st March will not count against the practice achievement as an automatic PCA will be applied.
In the Indicator Navigator folder, PCIT has provided searches for patients who have received only one invitation and are still outstanding. Once a second invitation has been sent to everyone on this list then there should be very few patients left outstanding on the indicators listed here.
IMPORTANT – HI03 for LD Heath Checks does NOT have an exclusion rule for invitations. The only PCA for this indicator is that the health check has been explicitly declined by the patient or an appropriate 3rd party.
For this indicator it is again important to start with the Data Quality report and ensure that all health checks have been fully coded.
Once the Data Quality work has been completed, there is a search to identify all remaining patients who are outstanding a LD health check in 025B PCN DES / 025B PCN DES Health Inequalities / Work to do | Needs LD health check.
These patients are likely to need individual consideration rather than bulk text invites as they may have flags or alerts for reasonable adjustments. Patients on this register are also at higher risk for safeguarding concerns so any patients who have not responded at all to invitations may need to be considered in this light. A useful option can be to reach out to other agencies involved such as the Community LD Team or discuss patients at multidisciplinary meetings as there may be alternative options for discussing the review with the patient or their carer.
Remember that LD health checks are also part of an ES which has a separate payment per health check. This means practices may wish to prioritise completing outstanding health checks before 31st March to achieve this additional funding.
Consider Quick Wins
The main Quick Win for these indicators will be the Data Quality searches as these ensure the practice is paid for work that has already been done.
DEM004 – practices may wish to consider whether the patient has had an appointment with a GP which has not been explicitly coded as a dementia care plan review, but which covered all the requirements for this review. The DEM | REVIEW | Had appointment this year but dementia review not coded search in Indicator Navigator helps identify patients who have had an appointment during the QOF year, but dementia review has not been coded.
Consider PCAs Understanding and applying PCAs appropriately can often be the difference between practices achieving maximum QOF points for an indicator and failing to get those last few points.
PCAs include:
o 2 invites sent with no response
o Informed dissent
o Clinically unsuitable
Invitation PCAs – it is always important to ensure that QOF related invitations are appropriately coded. As long as a patient has had 2 invites (using an appropriate code) which were added at least 7 days apart during the QOF year, there is no need to manually add a PCA. The 2 invites will automatically be applied as a PCA. Remember this does NOT apply to HI03 as the LD health checks are an IIF indicator and have different rules to the QOF indicators.
When sending invitations, it is important not to keep sending invitations to all outstanding patients, especially in Q4 when the practice is likely to have limited capacity for reviews. Make sure that patients are only being booked for review appointments if they have not already had the work done earlier in the year. If sending invitations based on a birthday month system, practices should check they have a plan to ensure that patients with a birthday in March receive invitations in sufficient time to be seen before 31st March and that patients with a birthday in April who have already been reviewed in April 2025 do not receive invitations too soon and end up booked in March 2026.
Final Tips
Remember:
·Have a clear plan
· Know the targets
· Identify outstanding patients
· Consider quick wins
· Consider PCAs
Check out the PCIT support articles for detailed support for each indicator and a full list of useful code
📹 Thank you to everyone who joined us for our “Wondering about QOF at this time of year?” webinar. For customers, this was a refresh of our GP Contract Pro tools, particularly focusing on actions to tidy up QOF at this time of the year.
This webinar showed PCIT resources but is suitable for both customers & non-customers utilising either EMIS Web or TPP SystmOne.
🌐 Watch here: Wondering about QOF at this time of year? on Vimeo