Achieving Time Sensitive Indicators
Introduction
Many practices struggle to achieve full points on time sensitive indicators because there is a limited time to complete activity and once that time has passed, that patient is likely to be excluded. These are also indicators that tend to have smaller parent populations which means that one or two patients can make a significant difference to achievement and income. Although it is not possible to go back in time and complete missing activity, it is still worth reviewing these indicators in Q4 as often there are patients where the activity has been completed but not coded. A feature of time sensitive indicators is that patients are not included in the system supplier’s denominator searches until they have achieved the indicator or the timeframe for completing the indicator has elapsed.
The Indicators:
Support articles for these indicators include comprehensive information on achieving the indicators and useful codes:
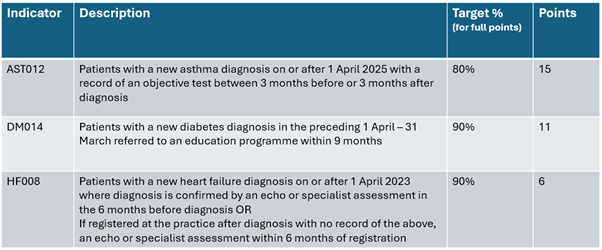
AST012 – Newly diagnosed asthma with tests
DM014 – New diabetics referred to Structured Education Programme
HF008 – New Heart Failure diagnosis with echo or specialist assessment
AST012 – Asthma Diagnosis

This indicator was new for 2025/26 following guidance published in November 2024. It contains some significant changes over its predecessor AST011, removing the requirement for spirometry while accepting a range of tests such as FeNO, FBC blood test (for eosinophils), bronchial challenge and skin prick tests (the latter for under 16s only).
AST012 did reduce the time frame for testing compared to AST011 so it is important for the team to be aware of this as adding a diagnosis too early or too late can cause patients to be excluded.
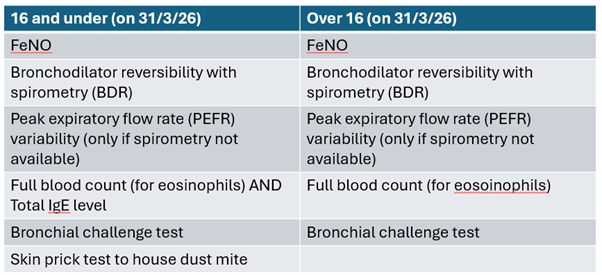
It should be noted that the requirements for under 17s is based on the patient’s age on 31ST MARCH 2026. This means a patient may have been aged 16 when a skin prick test or IgE level was done, but they would fail the indicator because they turned 17 before 31/03/26. Clinicians may need to be aware of this when considering the appropriate diagnostic test for a patient.
Things to remember
– Patients diagnosed or registered in the last 3 months of the QOF year (on or after 01/01/2026) will not count against the practice for the current QOF year if no objective tests are done. The newly diagnosed patients will be included in the 26/27 QOF year so it is important to ensure they still receive diagnostic testing within the required timeframe.
– If peak expiratory flow rate (PEFR) variability is used as the diagnostic test then there also needs to be a code on the patient’s record showing that spirometry was not available.
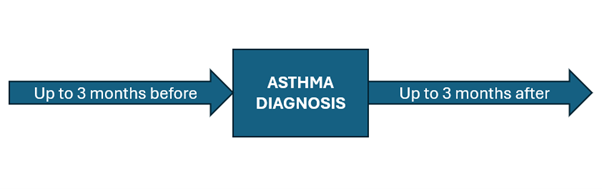
– This indicator looks for objective tests between 3 months (93 days) before to 3 months (93 days) after the diagnosis. For diagnosis it looks for the earliest code indicating an asthma diagnosis.
– If a patient appears on the indicator but has an older diagnosis of asthma on their record this is usually due to an ‘asthma resolved’ code. If a patient is coded as Asthma resolved and then seen and coded again with Asthma this will count as a new diagnosis. Clinicians should be aware of this as they may need to repeat diagnostic testing following this new diagnosis.
– In most cases a patient will be coded as Suspected asthma, so diagnostic testing will be done and then a diagnosis of Asthma will be confirmed and coded if appropriate.
– If a patient has been coded with Asthma before diagnostic testing is done, this can mean the patient ends up breaching the 3 month target for various reasons. This is especially likely where practices have limited capacity to perform tests such as FeNO or spirometry.
– When looking at excluded patients it is important to check the codes used for the tests and for the diagnosis.
– Patients diagnosed or registered in the last 3 months of the QOF year (on or after 01/01/2026) will not count against the practice for the current QOF year if no objective tests are done. The newly diagnosed patients will be included in the 26/27 QOF year so it is important to ensure they still receive diagnostic testing within the required timeframe.
Check the PCIT support article for all the essential codes and criteria AST012 – Newly diagnosed asthma with tests
DM014 – Diabetes Diagnosis
DM014 is a longstanding indicator so the practice team should be familiar with the requirement, especially those responsible for diagnosing and supporting new diabetics.
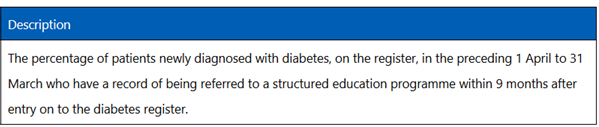
The indicator looks for a code that indicates the patient was referred to an education programme, it does not require evidence that the patient has completed it.
It only looks for a referral AFTER the patient has been added to the diabetes register.
The wording of DM014 can be misleading as it mentions patients newly diagnosed in the preceding 1 April to 31 March BUT it actually looks at patients diagnosed up to 21 months before the end of the QOF year.
This means that patients diagnosed between 1st July 2024 and 31st March 2026 are potentially eligible.
Patients who were diagnosed in the last 9 months of the current QOF year but who have not yet been referred to an education programme will not count against the practice as they can potentially be included in the next QOF year.
Whether a patient counts for the 24/25, the 25/26 or the 26/27 QOF year will depend on the date of diagnosis AND the date of referral.
Things to remember
– There are a number of structured education programmes that count for DM014 – see the PCIT support article for the full list of codes.
– If the practice has referral forms or letters saved as document templates, ensure the correct referral code is attached to that template so it is automatically added when that form or letter is used.
– There are also PCAs for a patient declining a referral or failing to respond to invites for a diabetic review appointment.
For more tips and codes see the PCIT support article – DM014 – New diabetics referred to Structured Education Programme
HF008 – HF Diagnosis
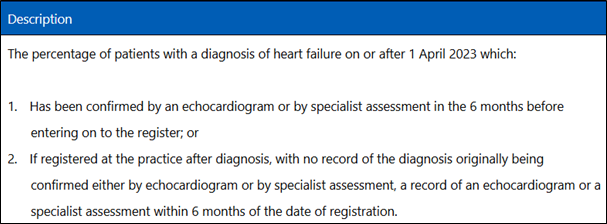
HF008 looks at patients diagnosed on or after 1st April 2023. This means that patients who fail the indicator can affect QOF achievement for multiple years.
The requirement is an echocardiogram, a specialist assessment OR an appropriate referral. It often reflects work done in secondary care rather than work done by the practice so accurate coding of letters or discharge summaries can be especially important here.
The echocardiogram, assessment or referral must be BEFORE OR ON THE SAME DAY as the earliest unresolved diagnosis of heart failure.
Things to remember:
– Patients who register at the practice with a diagnosis of HF since 1 April 2023 should either have the appropriate codes added to their record based on available correspondence OR an appropriate code to indicate if there was no appropriate service.
– Heart failure is often diagnosed in secondary care – make sure your admin/coding team is aware of the requirements for QOF and the appropriate codes.
– A Referral for echocardiography code can count for this indicator. So even if patient has been diagnosed during an inpatient stay and diagnosed with an outpatient referral for cardiology, or for testing, the referral itself will count IF coded ON OR BEFORE the date of diagnosis
– Patients who register at the practice with a diagnosis of HF since 1 April 2023 should either have the appropriate codes added to their record based on available correspondence OR an appropriate code to indicate if there was no appropriate service.
– Patients who register in the last 6 months of the QOF year will not count against the achievement in the current QOF year.
– Practices should have a process for identifying patients with HF when they register and checking that they have appropriate codes in their record once the electronic transfer/GP2GP has been received or checking paper records once received if electronic transfer was not possible.
– Patients diagnosed or registered in the last 3 months of the QOF year will not count against the achievement in the current QOF year.
For more tips and codes see the PCIT support article – HF008 – New Heart Failure diagnosis with echo or specialist assessment
Final Tips
– Ensure the practice team is aware of the importance of currently coding diagnostic tests, referrals and diagnoses for these disease registers.
– Codes such as Suspected asthma and Suspected heart failure may be more appropriate to use prior to diagnostic testing than adding a diagnosis that has not yet been confirmed.
– Ensure staff dealing with incoming letters or discharge summaries recognise new diagnoses that may need to flagged with a clinician, and use appropriate dates and codes.
– Ensure those dealing with new patient registrations/records or summarising are aware of the need to identify patients recently diagnosed with asthma, diabetes or heart failure so that coding can be reviewed in case tests or referrals are outstanding.
📹 Thank you to everyone who joined us for our “Wondering about QOF at this time of year?” webinar. For customers, this was a refresh of our GP Contract Pro tools, particularly focusing on actions to tidy up QOF at this time of the year.
This webinar showed PCIT resources but is suitable for both customers & non-customers utilising either EMIS Web or TPP SystmOne.
🌐 Watch here: Wondering about QOF at this time of year? on Vimeo