Using our Searches to Maximise QOF Potential in Q4
Introduction
This article follows on from Planning to Maximise your QOF Potential in Q4, where we focused on identifying missing income, prioritising indicators and creating a clear practice action plan. This second guide is about delivery. Once priorities are agreed, practices need a structured way to work through outstanding QOF activity efficiently, avoid wasted effort, and focus clinical time where it will have the greatest impact. PCIT’s 004B Routine QOF folder is designed specifically to support this stage of work.
What is the 004B Routine QOF folder?
The 004B Routine QOF folder was fully refreshed for 2025/26 and provides a comprehensive set of searches and reports to support day-to-day QOF delivery, particularly in Q4. Unlike high-level performance monitoring searches, 004B focuses on: Live, actionable patient lists, identifying incomplete or missing coding as well as targeting borderline patients and quick wins and supporting appropriate and safe use of PCA exclusions. For Q4 work, PCIT recommends using the searches in the 004B folder rather than population-excluded lists from 004A searches or Optum QOF searches when establishing true work outstanding.
When should practices use 004B during Q4? 004B is most effective when used throughout Q4, with a slightly different focus as the quarter progresses:
– Early Q4 (January) – Establish true work outstanding, clean denominators, and issue outstanding invitations.
– Mid Q4 (February) – Focus on data quality, incomplete reviews, borderline patients and quick wins.
– Late Q4 (March) – Final mop-up of high-value indicators, CV Focus work and PCA reviews.
This staged approach helps ensure clinical and administrative effort is targeted appropriately as time becomes more limited.
Overview of the 004B folder structure: The 004B Routine QOF folder is divided into 11 main folders, covering all major QOF indicator areas. Two folders are particularly important in Q4: Indicator Navigator and CV Focus. The PCIT 004 support article provides a full breakdown of all folders. This guide focuses on how to use the most impactful areas during Q4.
Indicator Navigator – the core Q4 delivery tool
The Indicator Navigator folder provides live, indicator-specific lists designed to help practices: Track outstanding work, resolve incomplete coding, identify high-risk or disengaged patients, manage PCA opportunities, target borderline and quick-win patients and practices should work through each Indicator Navigator folder in a structured order, rather than dipping in and out. Recommended order of work: Invitations > Data quality / incomplete reviews > High-risk and disengaged patients > PCA checklists > Borderline and quick-win lists. This mirrors how work is most efficiently delivered in real practice settings.
Invitations – clarifying true work outstanding
What these searches show : Patients who require invitations to support QOF exclusion rules. Why this matters in Q4: Two valid invitations (with appropriate invite codes) issued at least 7 days apart exclude patients from the denominator and this helps practices understand true work outstanding and avoids chasing patients who will not affect achievement.
Key points:
– Once two valid invitations are recorded, patients are automatically excluded
– If a patient later attends and meets indicator requirements, they will be included
– For BP, HbA1c and cholesterol indicators, the invitation count resets if a new high result is recorded
PCIT recommendation : Aim to issue second invitations by the end of January, giving the practice a clear picture of achievable work for the remainder of Q4. PCIT support articles list all correct invite codes for each indicator to ensure exclusions apply correctly.
Data quality and incomplete reviews – avoiding wasted appointments
What these searches show: Patients who have partially completed a review or check but are missing one or more required codes. This is particularly common for: Asthma, COPD, Heart failure, Learning disability health checks. Why this matters in Q4: Patients may have attended for a review but still not count for QOF, leading to: duplicate invitations, frustrated patients and wasted clinical time. In EMIS, associated reports show which codes have already been entered, making it easier to identify what is missing.
PCIT recommendation: Action these searches regularly throughout Q4 to ensure completed work is correctly reflected in QOF achievement.
High-risk and disengaged patients
What these searches show: Patients who are not responding to invitations, may be high clinical risk and are prescribed medication for the condition. Why this matters in Q4: These patients may be at higher risk of: Unplanned admissions, A&E attendance and urgent home visits. Practices may wish to prioritise review or proactive management even if QOF achievement is uncertain.
PCA checklists – supporting safe exclusions
What these searches show: Patients who may be appropriate for PCA exclusions based on clinical context.
When these are most useful:
– Early Q4: to avoid inviting patients who are clinically unsuitable
– Mid–late Q4: to review patients already known to clinicians due to frailty, co-morbidities or maximum tolerated therapy
– These patients are often already seen regularly and can benefit from holistic review rather than repeated QOF-focused invitations.
Borderline and quick-win lists – maximising points efficiently
What these searches show: Patients who are close to meeting indicator requirements or where a single action could trigger achievement. Why this matters in Q4: These lists often deliver the highest return for the least effort, particularly earlier in the quarter.
Examples:
– Patients missing a BP this year but with a previously normal reading
– Patients on alternative lipid-lowering therapy without a coded reason for not taking a statin
– Patients just outside target ranges
– Practices that collect large volumes of home BP readings may also find patients narrowly missing targets due to home BP adjustments. Inviting these patients for an in-practice reading can often convert them into achievement.
CV Focus – protecting high-value QOF income
The CV Focus folder supports BP and cholesterol indicators where patients may appear across multiple indicators. This is particularly important in 2025/26, as QOF funding has shifted from disease registers towards cardiovascular indicators. For the average practice, under-performance here can risk around £10,000 of QOF income.
What CV Focus helps practices do
– Identify patients affecting multiple BP indicators
– Prioritise high-value actions
– Avoid duplication across indicators
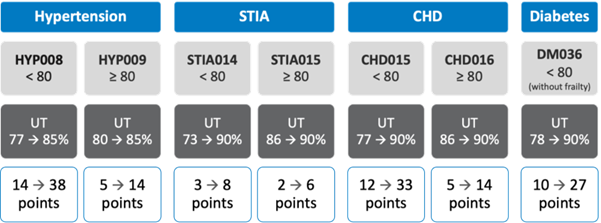
Practices may wish to prioritise:
- CV | 4 BP indicators outstanding
Patients whose BP, once in range, will affect four BP indicators simultaneously. - CV | BP last month not to target, no previous PCA, has new antihypertensives
Patients started on treatment after a high BP who may now be within target but lack a follow-up reading.
For each BP indicator, searches are provided covering:
– Borderline patients
– High-risk patients
– PCA review opportunities
– Quick wins
Cholesterol indicators
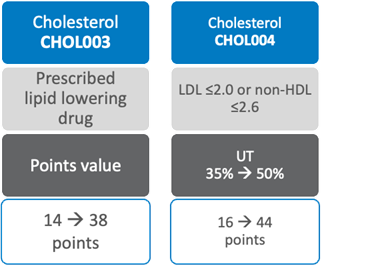
Common issues identified by practices include patients included in CHOL003 solely due to CKD coding where:
– Latest eGFR does not support CKD3–5
– Patients are over 80 with CKD only
– Relevant searches include:
- QUICK WIN CODING | CKD only reason for CHOL003 and normal eGFR
- QUICK WIN CODING | CHOL003 CKD only over age 80
A further common issue is use of statin-specific PCA codes rather than broader lipid-lowering therapy codes. These patients can be identified using:
- QUICK WIN CODING | Statin PCA this year but not wider lipid therapy PCA
For CHOL004, quick improvements can often be achieved by testing patients who were previously in range but lack a result this year:
- QUICK WIN VALUE | CHOL004 not on therapy, no result this year and previously normal
- QUICK WIN VALUE | CHOL004 on therapy, no result this year and previously normal
Borderline LDL cholesterol results can also be reviewed for potential titration or repeat testing.
Avoiding common Q4 pitfalls – The 004B folder helps practices avoid:
– Repeatedly inviting patients who already attended
– Overestimating achievable work
– Missing simple coding errors that block achievement
– Leaving high-value CV indicators until too late in the quarter
– Used consistently, it supports a calmer, more controlled Q4 approach.
What’s coming next in the series – This is the second in our series of Q4 QOF optimisation guides. Future articles will focus on:
– Indicator-specific deep dives
– Final Q4 mop-up strategies
– Avoiding last-minute data quality issues
Final note: The aim of 004B is not to increase workload, but to ensure that the work being done counts. Used alongside a clear plan, it helps practices maximise QOF achievement while making best use of limited clinical and administrative time in Q4.
Conclusion
This is the second in our series of regular articles which will offer Q4 tips for achieving maximum QOF points in a number of different areas using PCIT’s suite of resources.